
Could Blocking Brain Energy Sensing Kill You?
Lessons from a recent clinical trial blocking the body-to-brain hormone GDF15


ENERGY SCIENCE
In this post, Martin Picard and Alan Cohen discuss a recently published article about the risks of blocking a body-to-brain energy signaling hormone, GDF15. Here they unpack this idea in a more accessible way.
Over the course of millions of years, delicately balanced systems have evolved to manage our energy to best ensure survival.
For reasons that remain unclear, all animals, including humans have a limited energy budget.
To manage life with a cap on energy expenditure, our bodies have various systems in place to manage this budget and adapt during periods of high energy demand. These systems help keep critical functions running, and they prompt changes in our physiology and behavior to conserve energy when needed.
But what happens when we interfere with these energy management systems?
Signals for Maintaining Energy Balance
In a previous post, we described how our energy-hungry brains deal with a limited energy budget by changing how energy is allocated based on fluctuating energy demands. The brain monitors and manages bodily energy.
In the short term, this can get us through brief periods of heightened stress, but chronically high energy demands can affect the growth, maintenance, and repair processes that are essential for health and longevity.
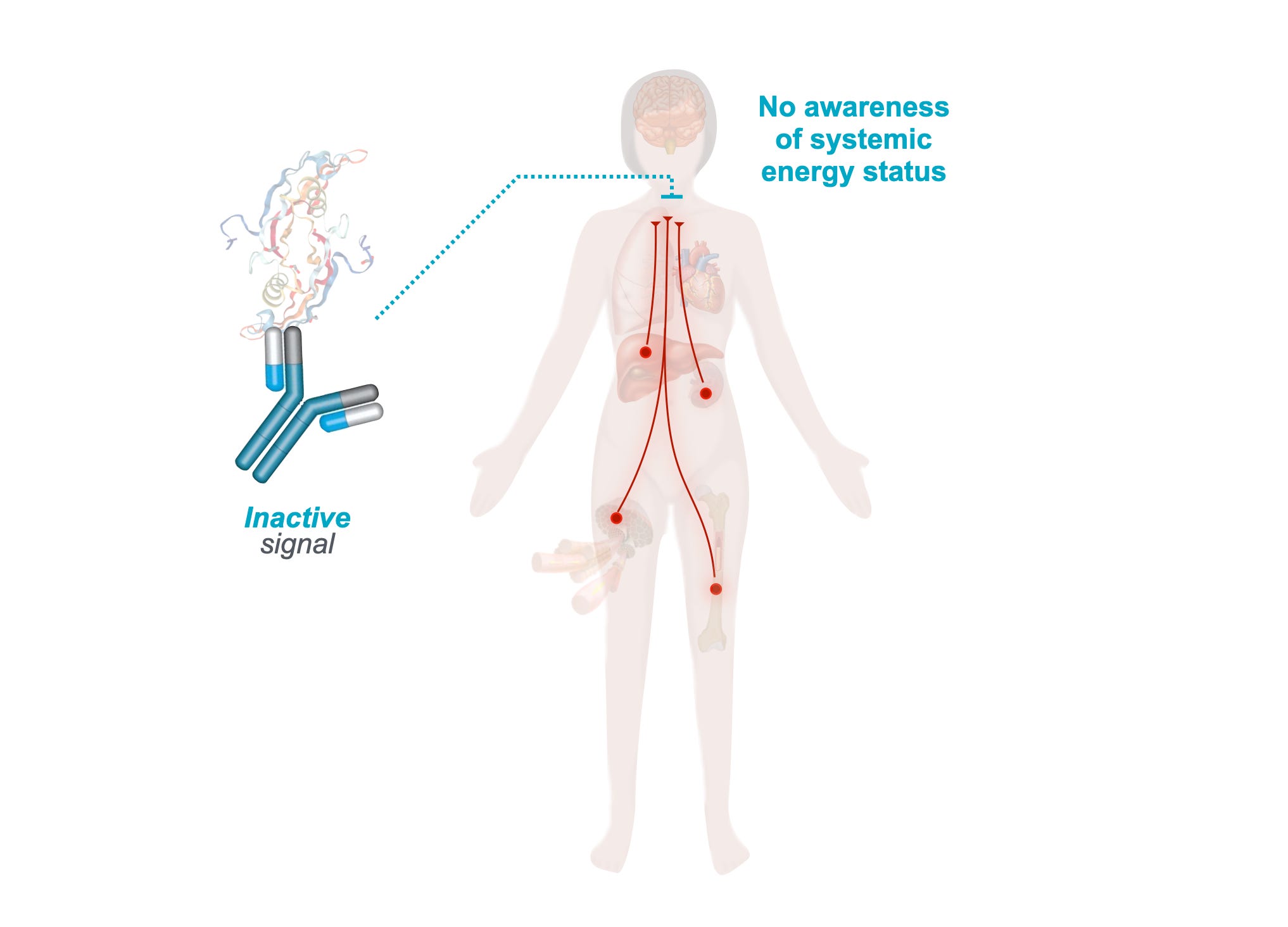
A key question then is: how does the brain “know” when we’re approaching our energy limit?
Growth differentiation factor 15 (GDF15) is a hormone and signaling protein released by cells under energetic stress, and it has emerged as a robust biomarker of illness. GDF15 levels correlate with disease, physical and cognitive disability, aging, and mortality.
We previously combed through the literature to understand what GDF15 means, and why it’s elevated in so many diseases. What we found links GDF15 to the health of mitochondria. And to their capacity to flow energy efficiently.

All sorts of stressors—physical and psychological—induce GDF15 we think by increasing energy resistance. In a preprint, we describe how stressors of all kinds converge on energy.
Looking at all of the correlations between high GDF15 levels and poor health, it can be tempting to believe that there is a simple solution. Can we just block GDF15 to fix these problems?
Unfortunately, biology is rarely that straightforward.
Short-Term Impacts of Blocking Brain Energy Sensing
Ponsegromab is a new drug that was developed to neutralize GDF15 to keep it from starting energetic stress-related signaling cascades in the brain.
At first glance, this approach makes a lot of sense. If GDF15 is linked to nausea, loss of appetite, weight loss, fatigue, and seemingly the general misery that can accompany serious illness, then blocking it might help people feel better. And in some short-term studies, that is exactly what results show.
For example, in a clinical trial of individuals with cancer and severe, unintentional weight loss, muscle wasting, and fatigue (a condition known as cachexia), taking ponsegromab for 12 weeks helped.
On average, patients in the group taking the highest dose of the drug had improved appetite, gained more weight, had reduced cachexia symptoms, and increased their physical activity.
For the patients in the study, these results may represent meaningful improvements in their daily life.
However, these short-term improvements may come at a cost.
Long-Term Considerations for Blocking Brain Energy Sensing
If GDF15 acts as an important distress signal that our brain uses to detect when our bodies are under severe energetic stress, blocking it could have some serious long-term consequences.
We recently published a commentary in the Journal of the American Geriatrics Society discussing the potential risks of blocking GDF15-based energy sensing in the brain.
Under energetic stress, the brain normally signals to the body to make changes to conserve energy. Activity drops, appetite is reduced, stress systems turn on, and energy is rationed and redirected to the functions most essential for our survival.
These compensations may not feel good, but they could potentially be life-preserving.
An analogy is the fiscal austerity of governments. When finances become too bad, cuts may be needed to some programs, but they may stave off worse consequences that would come if they were not made. When money or energy budgets are limited, hard choices may be necessary. (We say this as a general principle, without arguing that fiscal austerity was or wasn’t necessary in any given historical case.)
Blocking GDF15 might relieve some of the uncomfortable symptoms we experience while under energetic stress, but it may also blind our brains to the seriousness of our energy shortage.
This is why the short-term successes of GDF15-blocking therapies may not tell the whole story.
In the clinical trial for ponsegromab that we mentioned earlier, there were subtle indications that the treatment may have detrimental long-term effects. There were higher rates of severe adverse events and mortality in the groups that received ponsegromab (though these weren’t statistically significant).
This makes sense if we consider it in the context of our limited energy budget. For a patient with cancer, nausea and reduced appetite may be examples of how the body compensates to manage energy allocation. If a person is fasting, the portion of their energy budget that would typically be devoted to eating and digesting can instead be used for healing and supporting the immune system.

In fact, research has shown that beginning to feed critically ill children and adults with injected nutrients early during a stay in the intensive care unit (ICU) actually results in worse outcomes in both populations and increases mortality in adults. Waiting a week or more to start feeding may allow patients’ bodies to focus their limited energy on healing during the critical period after ICU admission.
Implications for the Future of Therapies Targeting GDF15
Emerging evidence about the potential long-term downsides of GDF15-blocking therapies doesn’t mean we should abandon them. Instead, we should be more careful with how they are used and for whom.
A treatment can improve symptoms in the short term while negatively impacting long-term health and longevity. That tradeoff may be acceptable in certain settings, especially in palliative care, where relief from nausea, weakness, or wasting may matter more than extending life. But outside of those settings, patients, families, and clinicians need more information to make informed treatment decisions.
A key take home message for medicine as a whole is that when we alter one piece of a complex system, there may be unexpected consequences that aren’t immediately apparent.
Our bodies work not like machines, but as dynamic systems that adjust and compensate for ongoing changes. All the parts are interconnected, and the response to a change we make in order to help could be the opposite of what we intend.
And let’s remember: nothing is free in biology; everything costs energy. So those adjustments and compensations come at a cost, too.
Sometimes the signals our bodies generate are unpleasant because the situation is dangerous. If GDF15 is part of the body’s survival strategy under extreme stress, then blocking it may be helpful in some ways but harmful in other ways.
Before anti-GDF15 drugs are embraced too broadly, we need larger studies with longer follow-up periods. And when evaluating these therapies, we need to adopt a wider lens that looks beyond immediate symptom relief to the harder question of whether patients are truly better off in the long run.
The energetic principle that applies in this case will apply to many other therapies too.
This case with GDF15 illustrates how randomized controlled trials - supposedly the gold standard for clinical evidence - are actually ill-equipped to detect the potential harms, particularly if the harms are off-target and longer term than the benefits
Curious about how energy impacts our bodies, minds, and experiences?
Visit our website to learn more.
Want to learn more about Intrinsic Health?
 | A guest post by
|
I agree that there are systems for detecting long-term or off-target harms, but they're harder to use because of the lack of clear control. This produces a ratchet effect where it's easy to approve new medications and indications and harder to see downsides.
RCTs are great tools when we have minimal a priori reason to suspect context-specific results, but should be used with particular caution when there is reason (like here) to explicitly predict trade-offs and/or divergent effects across temporal scales.
This post delineates what is to me the most revolutionary part of new mitochondrial science: energy allocation. We’ve long known mitochondria are responsible for energy production, but what do they DO with that energy, that, after all, is the purpose of the whole exercise. This opening chapter in that book is illuminating: GDF-15 resembles a fire alarm. Would we wish to unplug/suppress it just because it goes off ‘unpleasantly’? According to Martin, mitochondria aren’t just a power plant (that’s yesteryear), they’re a self-regulating system of computer controls navigating everything in the body which must not be unnecessarily disturbed, e.g. with GDF-15. This journey is starting to get really thrilling.